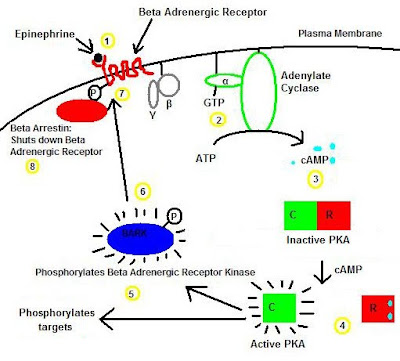
The basic pathophysiology of McCune-Albright syndrome starts with the G-protein intracellular signaling system. This is a ubiquitous signaling protein in many organs, including endocrine organs, that starts the cascade of activation via adenylate cyclase. For the unfamiliar, when a stimulator reaches a cell's receptor, that receptor triggers an intracellularly attached G-protein. This G-protein can activate adenylate cyclase in certain cells, and inhibits it in others. In cells that adenylate cyclase is activated, the resulting cAMP acts as a second messenger (G-protein being the first) by interacting with other proteins. Often, this leads to the production of proteins by the cell. In endocrine cells, cAMP is often the second messenger that is necessary to tell the cell to produce a hormone.
This picture is an example of cAMP activation from a beta-adrenergic receptor.
 In McCune-Albright syndrome, there is a somatic mutation (in other words, not inherited) which leads to uncontrolled activity of the G-protein. In short, the G-proteins start working even without a stimulus. The presentation of McCune-Albright syndrome will depend on where the mutation has decided to occur.
In McCune-Albright syndrome, there is a somatic mutation (in other words, not inherited) which leads to uncontrolled activity of the G-protein. In short, the G-proteins start working even without a stimulus. The presentation of McCune-Albright syndrome will depend on where the mutation has decided to occur.- Irregular cafe-au-lait spots (caused by autonomous production of melanin)
- Polyostotic fibrous dysplasia of the long bones (caused by autonymous activity of osteoblast progenitor cells)
- Precocious puberty (caused by GnRH-independent activtion of testes/ovaries)
- Hyperthyroidism
- Hyperadrenalism
- Acromegaly
3 comments:
Hello!
My 9 year old daughter has MAS/FD. I am wondering how many MAS patients you have treated? Our local PCP hasn't treated any other MAS patients, but has been amazing in his efforts to do as I ask, given my endless research and the requests of my daughter's many specialists. Also, have you been to the MAGIC Foundation's medical conference in Wheeling , IL?
It's wonderful to see others raising awareness of this rare and monstrous disease. Thank you for your time and attention to this. I wish you much luck in your work.
Warm Regards,
Tanya
Thank you Tanya for your comment. I am not an MAS specialist. I saw a patient with MAS during a volunteer medical mission.
My training is in pediatric critical care. My aim with this post is to make sure that general pediatricians don't just memorize the features MAS, but rather understand why they happen. In my practice, I like to understand as much as I can of an condition/syndrome/disease.
I commend your research into your daughter's condition, and I'm happy you found a pediatrician who has been helpful.
Good luck.
Here is a link to more information about the genetics of McCune-Albright Syndrome that was prepared by our genetic counselor and which has links to some useful resource for those dealing with this condition: http://www.accessdna.com/condition/McCune-Albright_Syndrome/728. There is also a number listed for anyone who wants to speak to a genetic counselor by phone. I hope it helps. Thanks, AccessDNA
Post a Comment